Acute renal failure, which often is a part of multi-organ failure with complications such as shock, cardial and non-cardial pulmonary edema, hemodynamic instability, bleeding, hypercatabolism
Non obstructive oliguria (u/o <200 ml/12 hr) or Anuria.
Severe Acidemia (pH <7.1) d/t metabolic acidosis
sepsis
Hyperkalemia (K >6.5 mmol/L)
Progressive severe dysnatremia (Na >180 or 115 mmol/L)
Suspected uremic organ involvement (pericarditis)
Drug overdose for dialyzable toxins
Hyperthermia (core temp. >39.5oC)
Clinical Conditions to Consider
ARF and need for fluid management related to
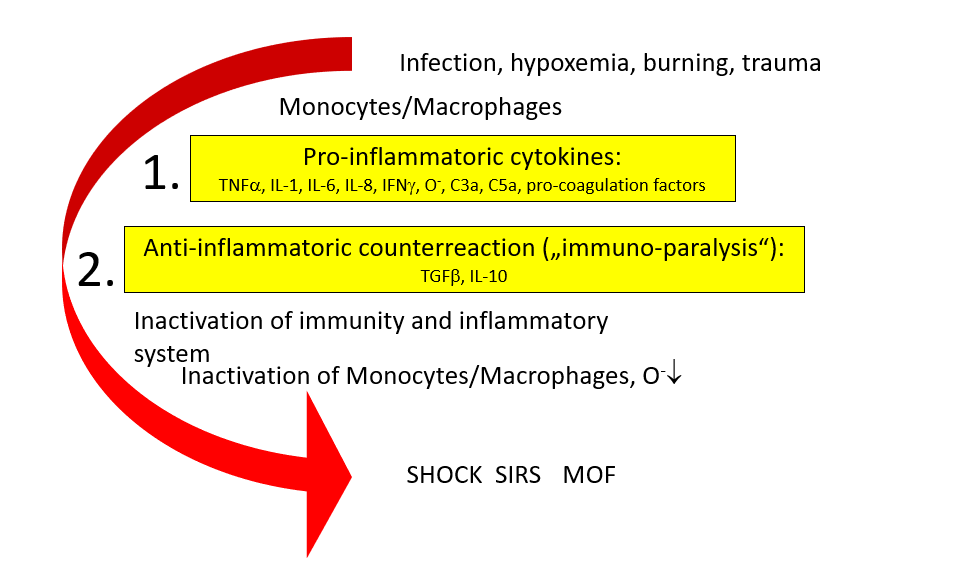
SIRS
Unstable on IHD
Organ transplants
CHF /volume overload
Post CV surgery
Post trauma patients
Severe Burns
What is Sepsis ? ACCP/SCCM Consensus Definitions
(ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. )
Severe Sepsis
Sepsis
Organ dysfunction
Septic shock
Sepsis
Hypotension despite fluid resuscitation
Multiple Organ Dysfunction Syndrome (MODS)
Altered organ function in an acutely ill patient
Homeostasis cannot be maintained without intervention
Infection
Inflammatory response to microorganisms, or
Invasion of normally sterile tissues
Systemic Inflammatory Response Syndrome (SIRS)
Systemic response to a variety of processes
Sepsis
Infection plus
۲ SIRS criteria
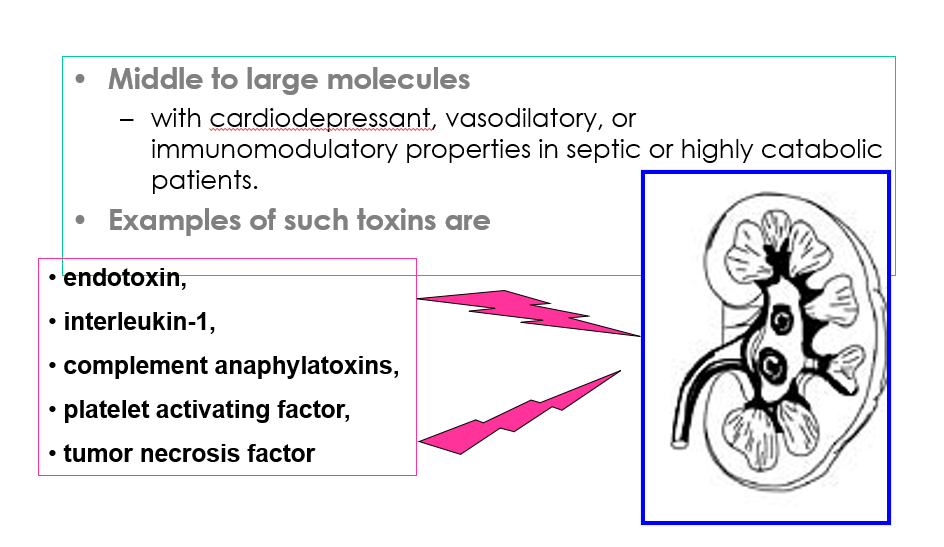
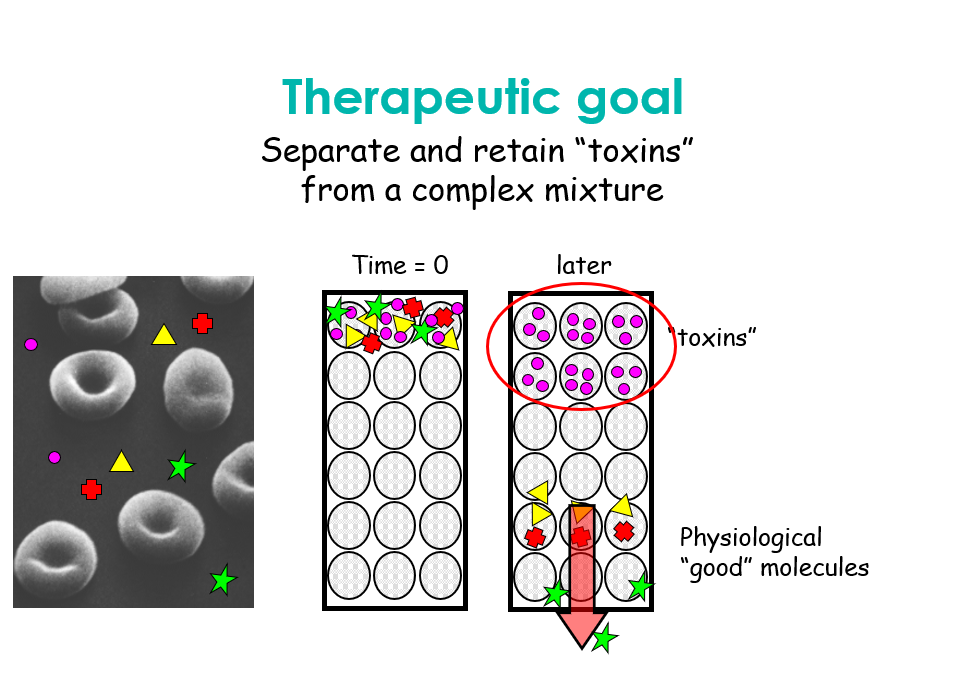
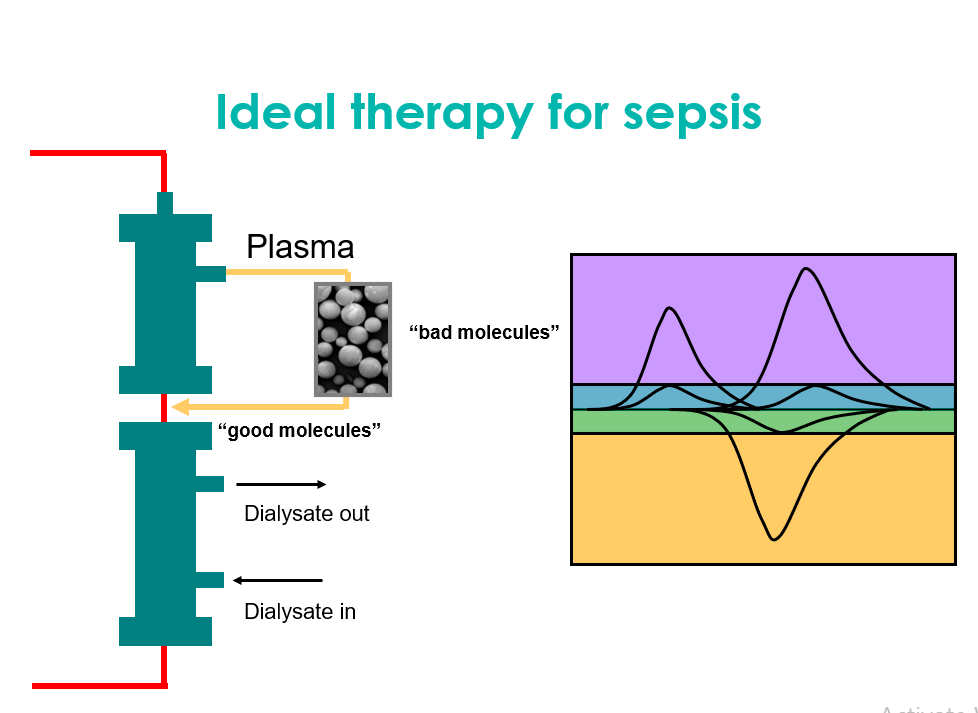
Removal of immunomodulatory substances in sepsis
Conclusion
Sepsis & SIRS
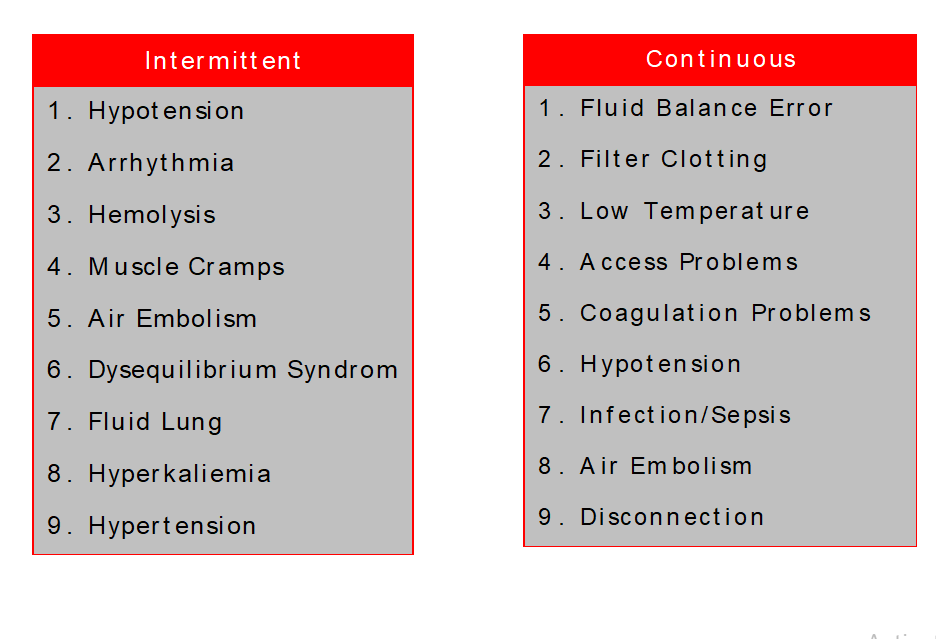
The most important complicationof intermittent hemodialysis
۱ – Hypotension % ۲۵ – ۵۰
۲ – Muscle cramp % ۵ – ۲۰
۳ – Arrythmia
Complications
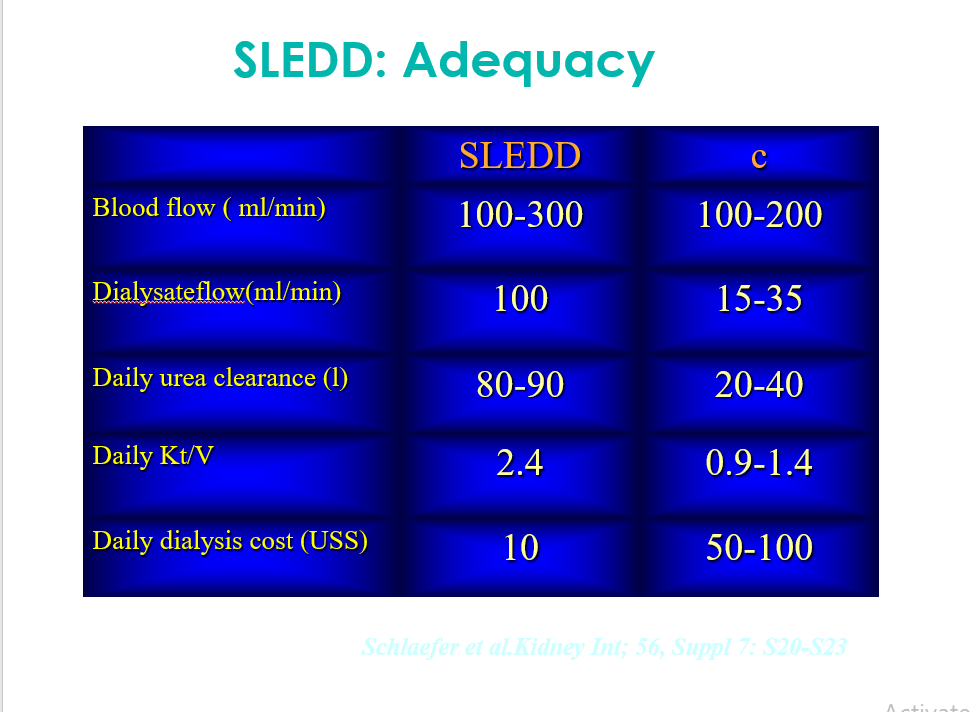
Suitable Dialysis
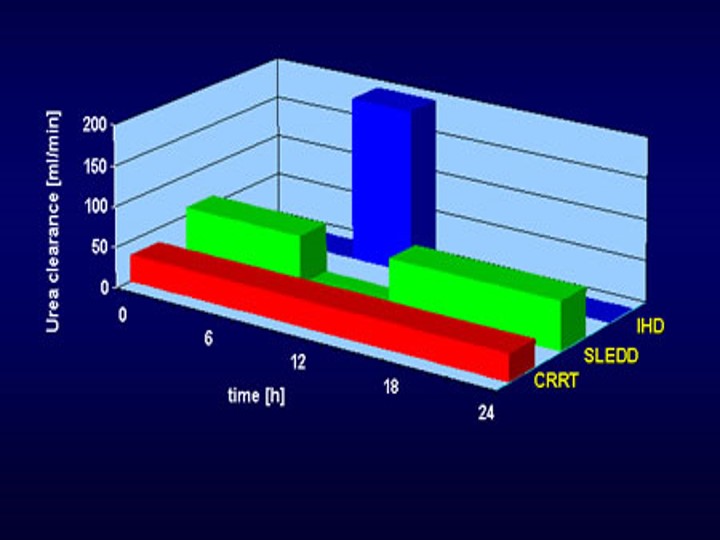
۱ – Better clinical tolerance
۲ – Better solute clearance
۳ – Improvement acid , base &
electrolytes
۴ – Biocompatibility
۵ – Minimum complications
۶ – Suitable monitoring during the
treatment
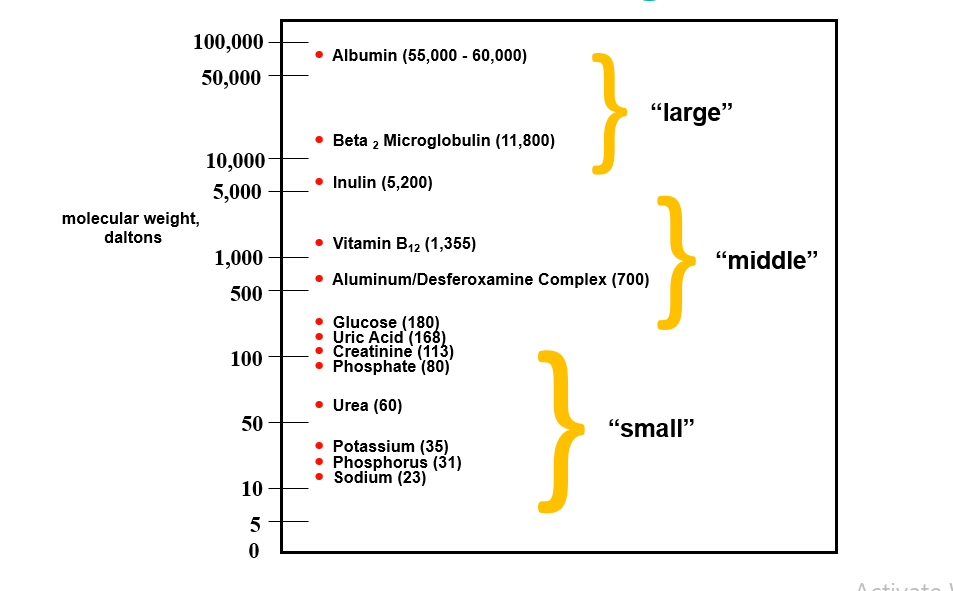
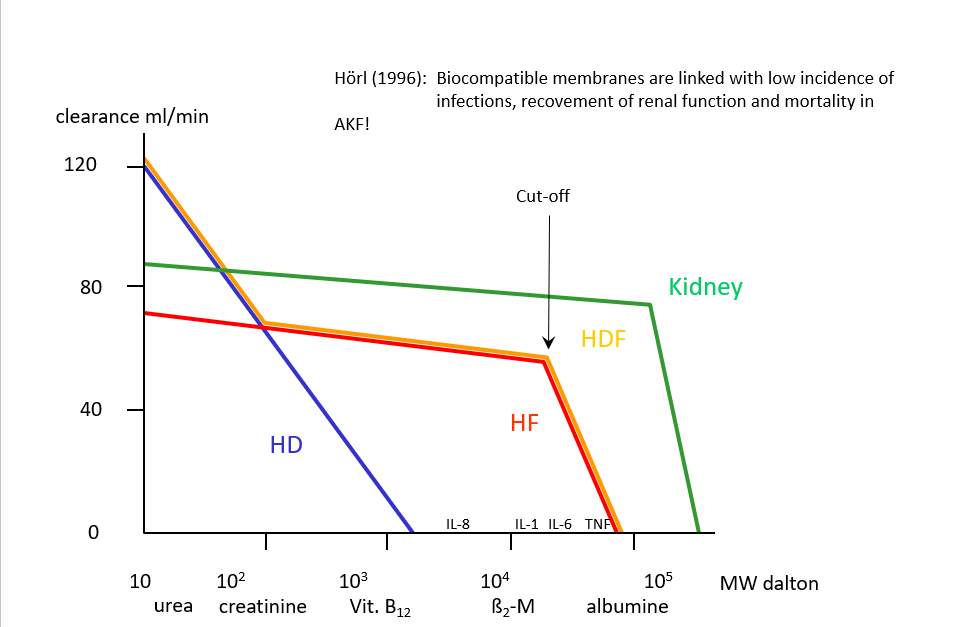
Molecular Weights
Terminology
Hemodialysis
transport process by which a solute passively diffuses down its concentration gradient from one fluid compartment (either blood or dialysate) into the other
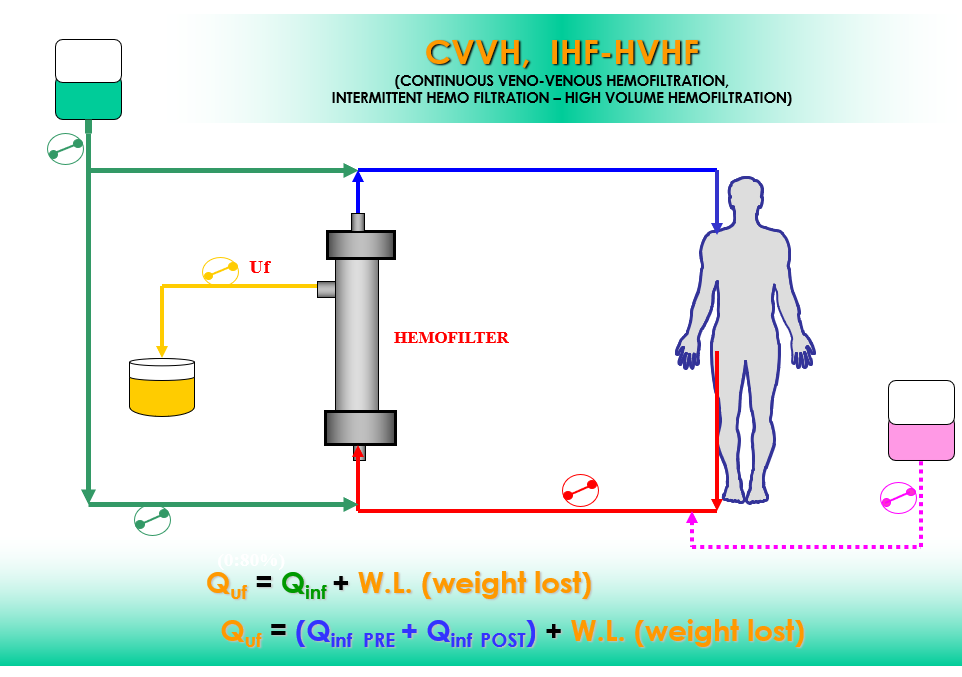
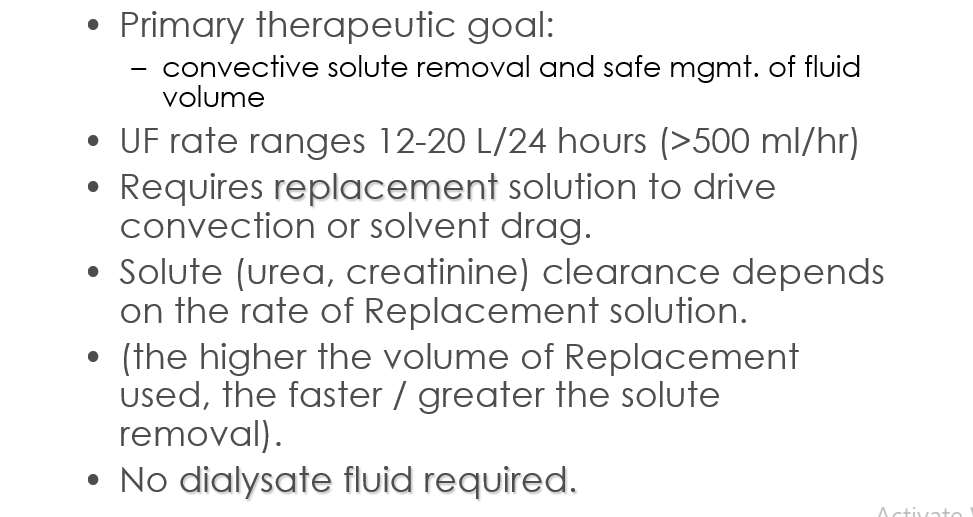
Hemofiltration
use of a hydrostatic pressure gradient to induce the filtration (or convection) of plasma water across the membrane of the hemofilter.
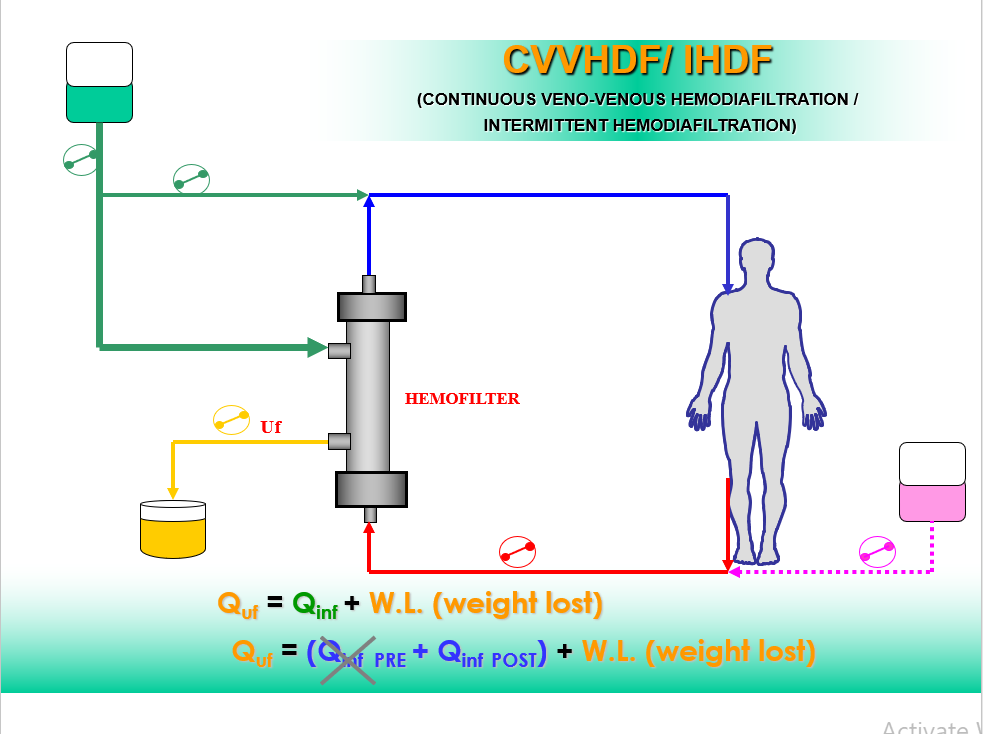
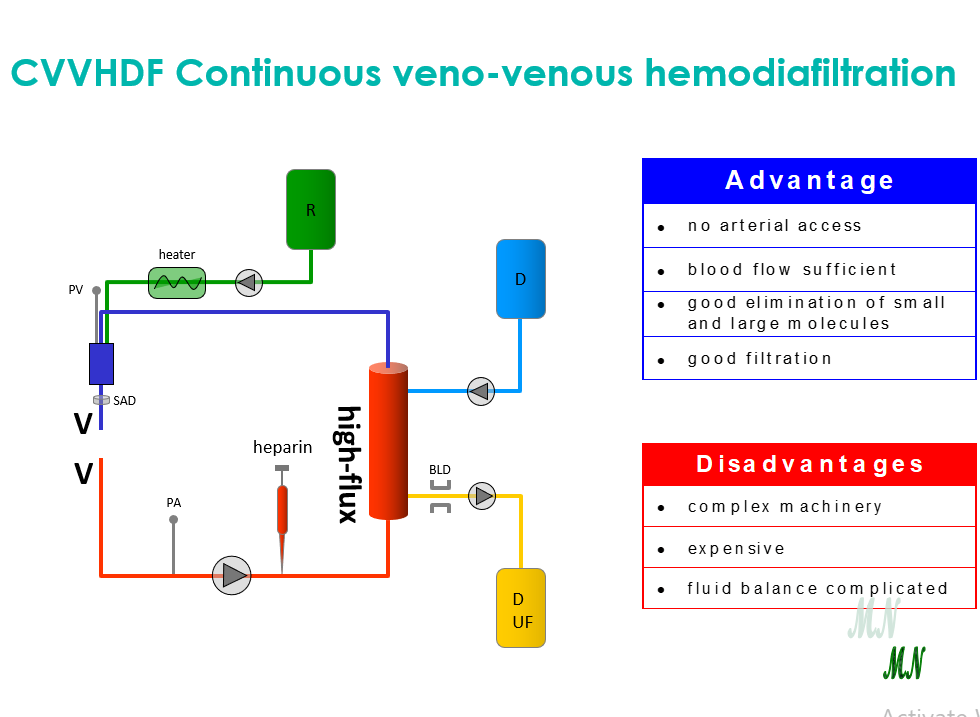
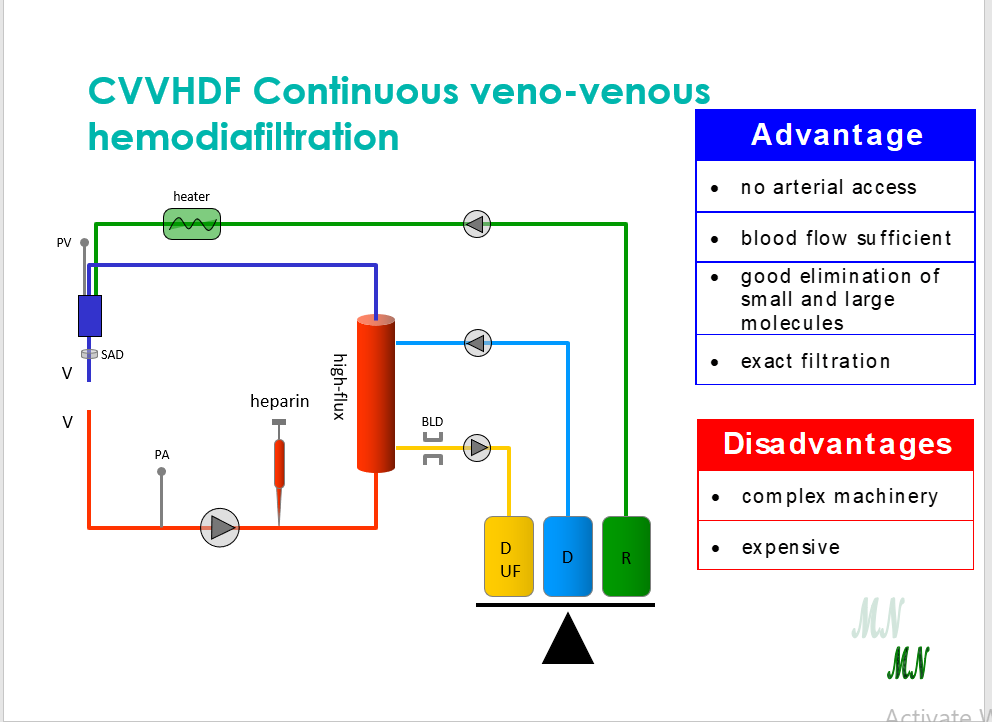
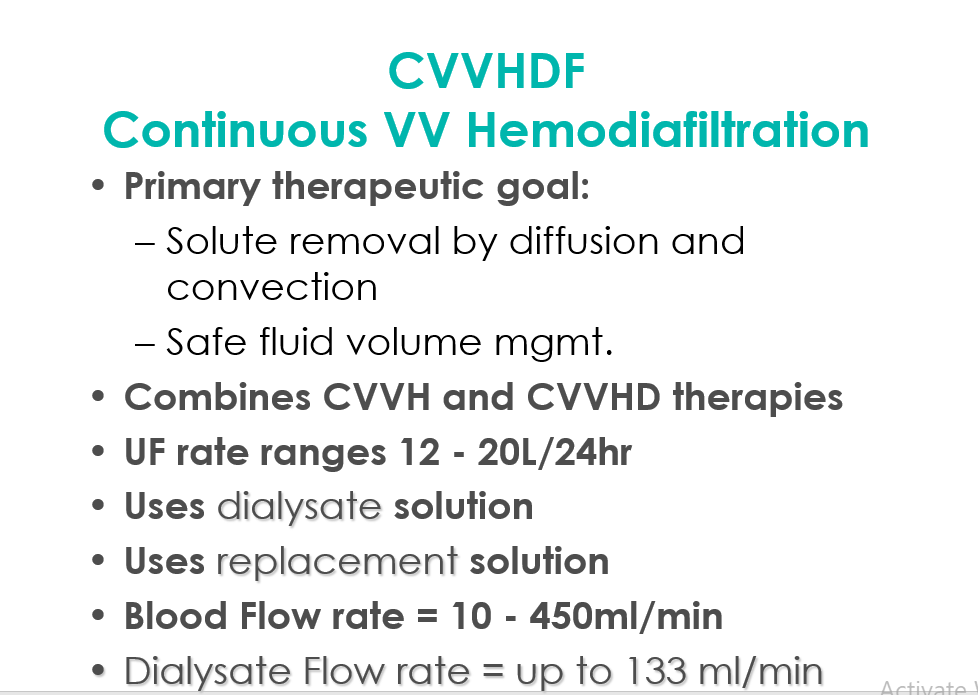
Hemodiafiltration
dialysis + filtration.
Solute loss primarily occurs by diffusion dialysis but 25 percent or more may occur by hemofiltration
Overview of CRRT
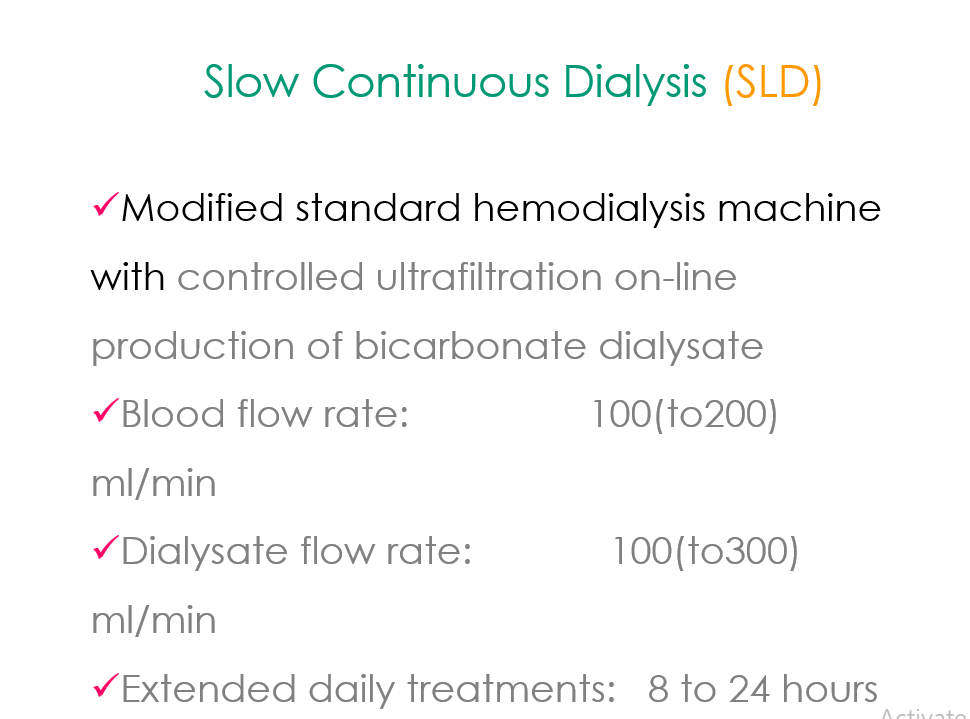
Slow Continuous Therapy
Low Blood Flow Rate
Low Dialysate Flow Rate
Low Replacement Flow Rate
Low Ultrafiltration Rate
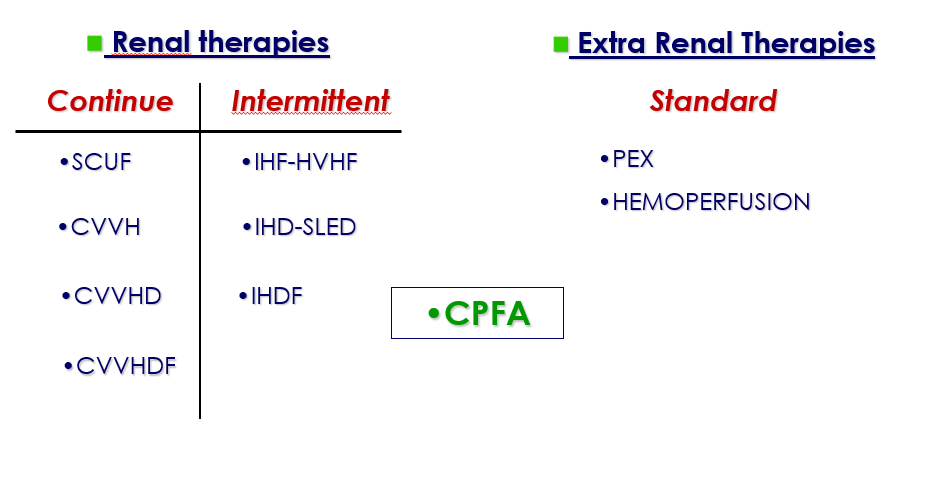
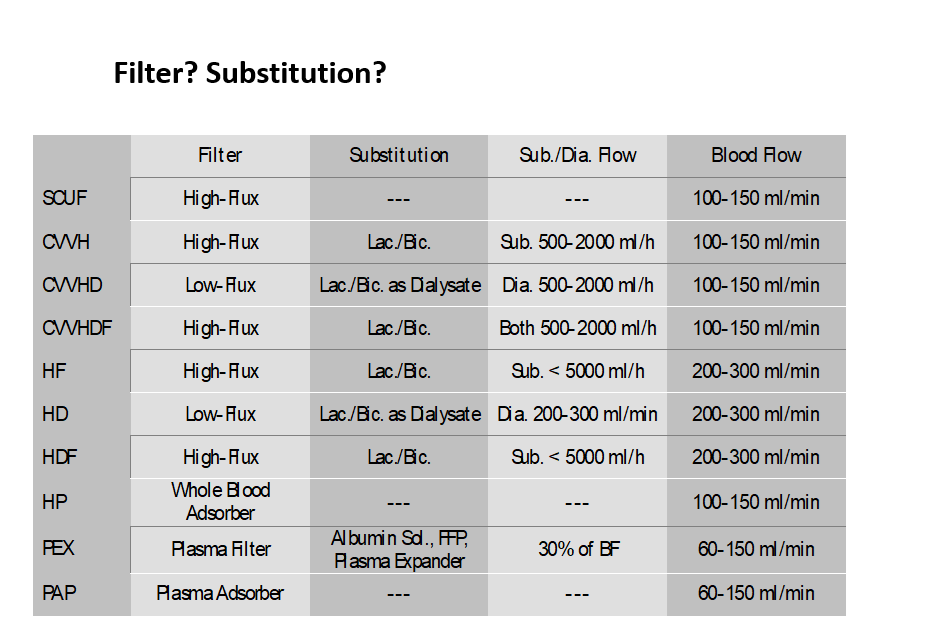
THERAPIES
Treatment Modalities
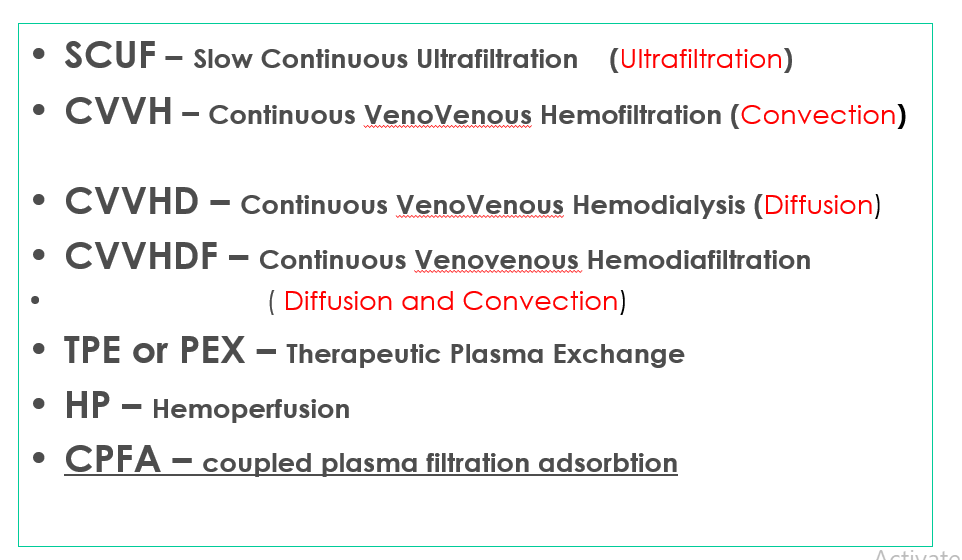
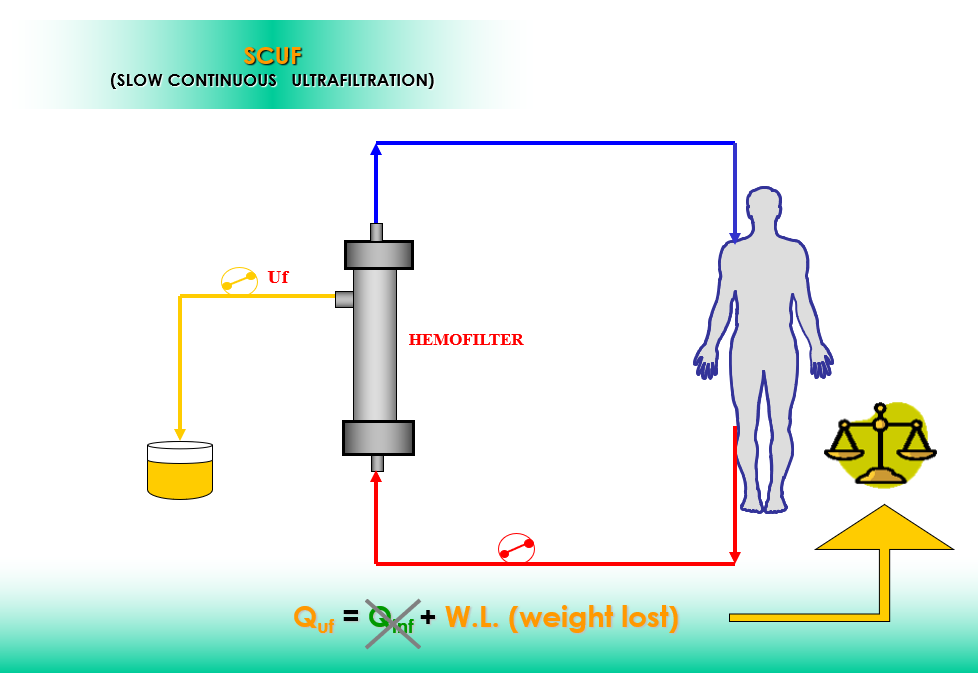
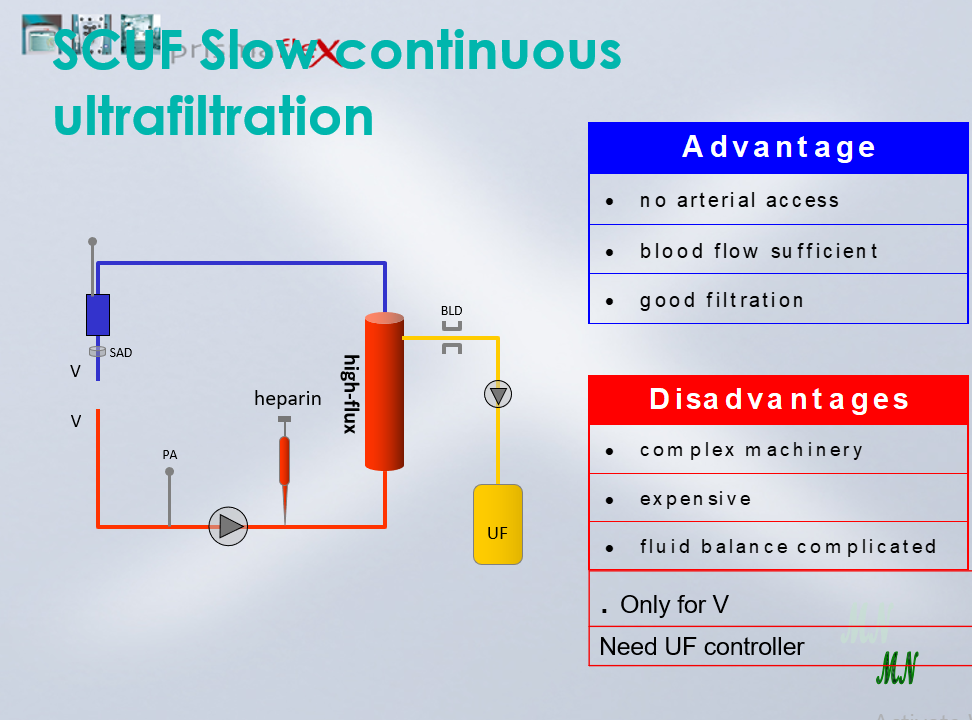
SCUF Slow Continuous Ultrafiltration
Primary therapeutic goal Safe management of fluid removal UF rate ranges up to 2 L/Hr No dialysate No replacement fluids Large fluid removal by ultrafiltration Blood Flow rates = 10 – 450 ml/min
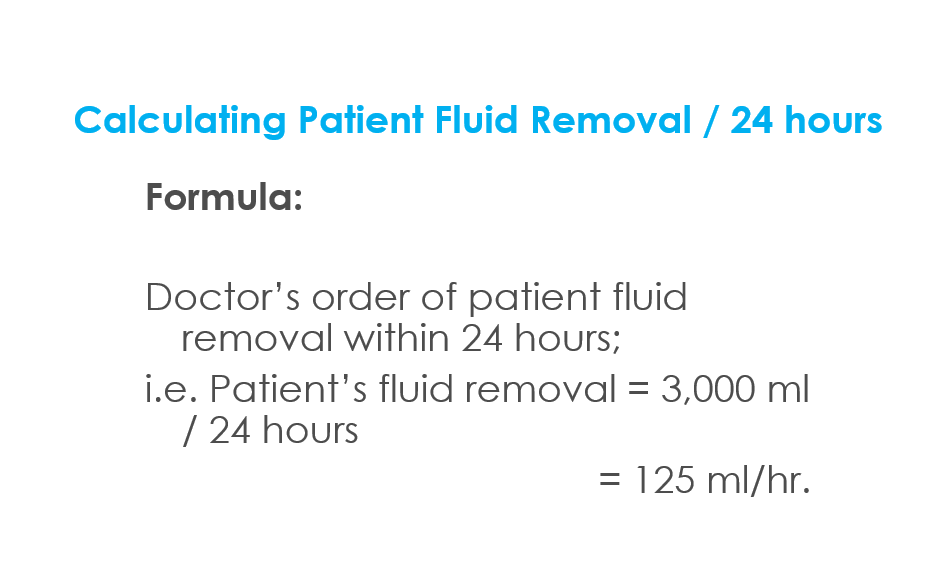
Goals of Fluid Management
Normovolemia Remove fluid to create a space for fluid therapy (24/7) Optimize hemodynamic parameters
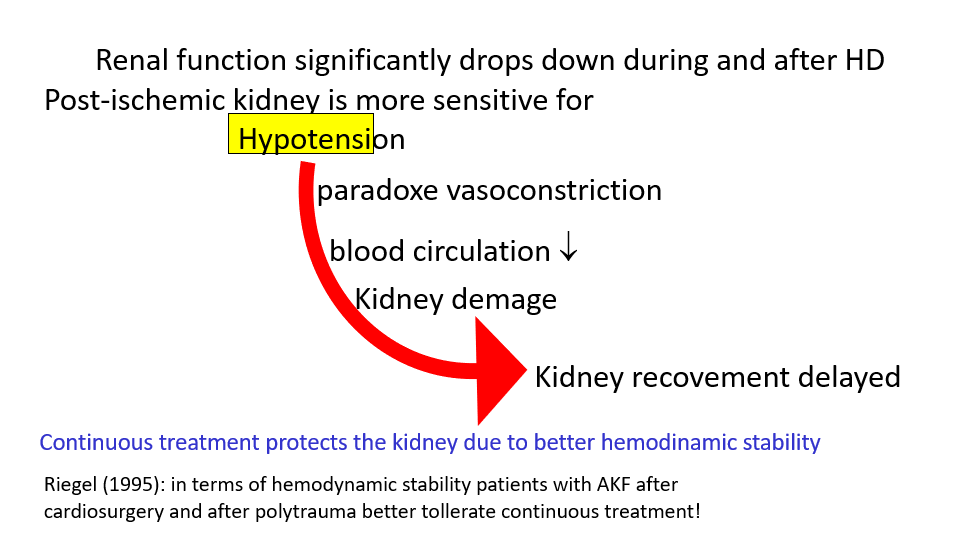
Avoid hypotension – drop down of systemic BP will cause marked fall in renal blood flow and will lead to further damage, insult or injury to kidneys
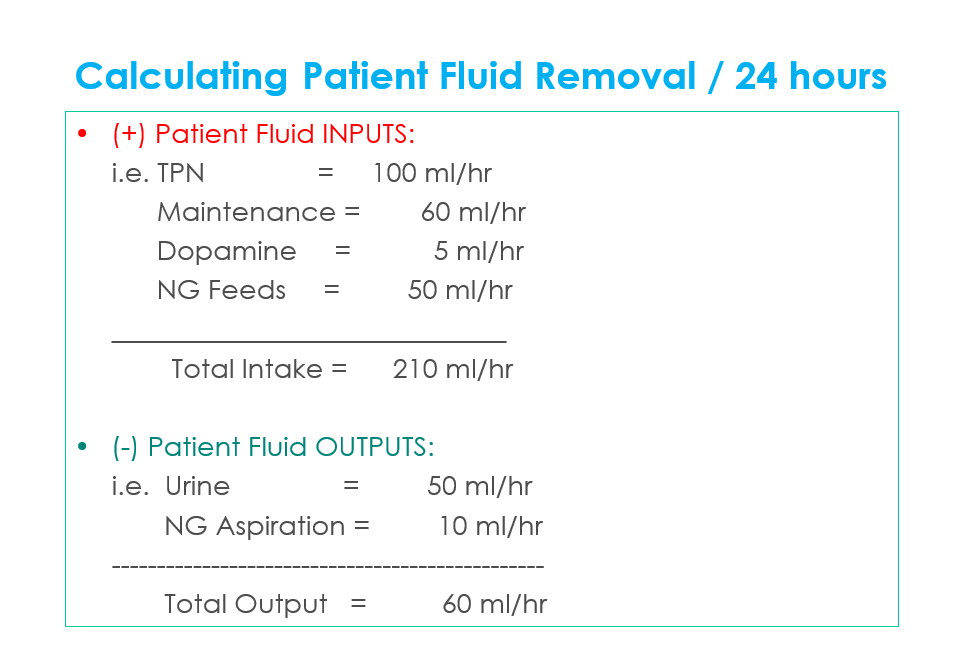
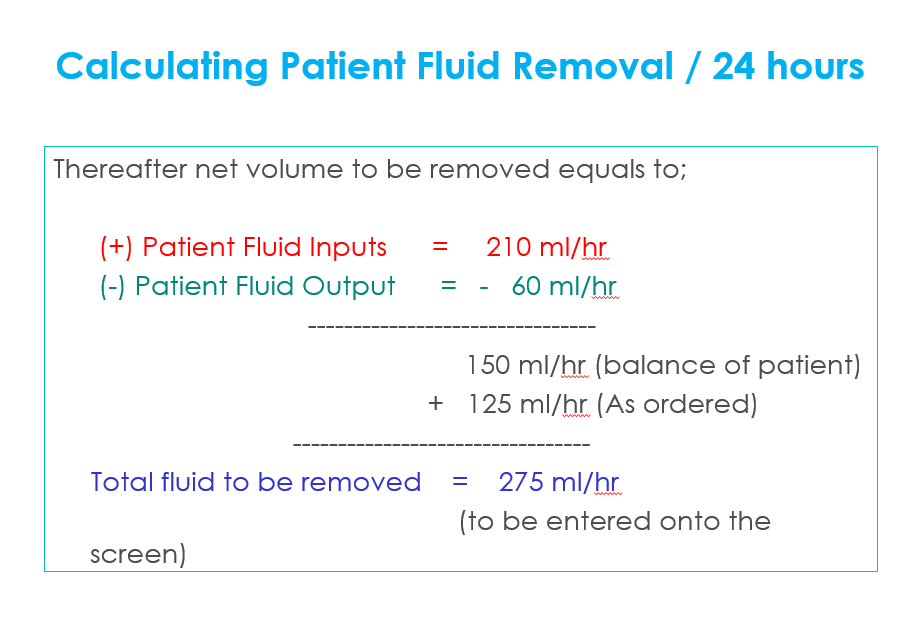
Fluid Management
Management
Monitor Intake & Output parameters on the status screen every hour of the machine Monitor the condition of the patient; – Excessive fluid loss, will lead to Hypotension and / or Hypovolemia
– Excessive fluid gain, will lead to Hypertension and / or Hypervolemia